

Intestinal Obstruction in a Toddler Due to a Meckel’s Band
A Case of Diagnostic Challenge and Successful Surgical Management
Abstract
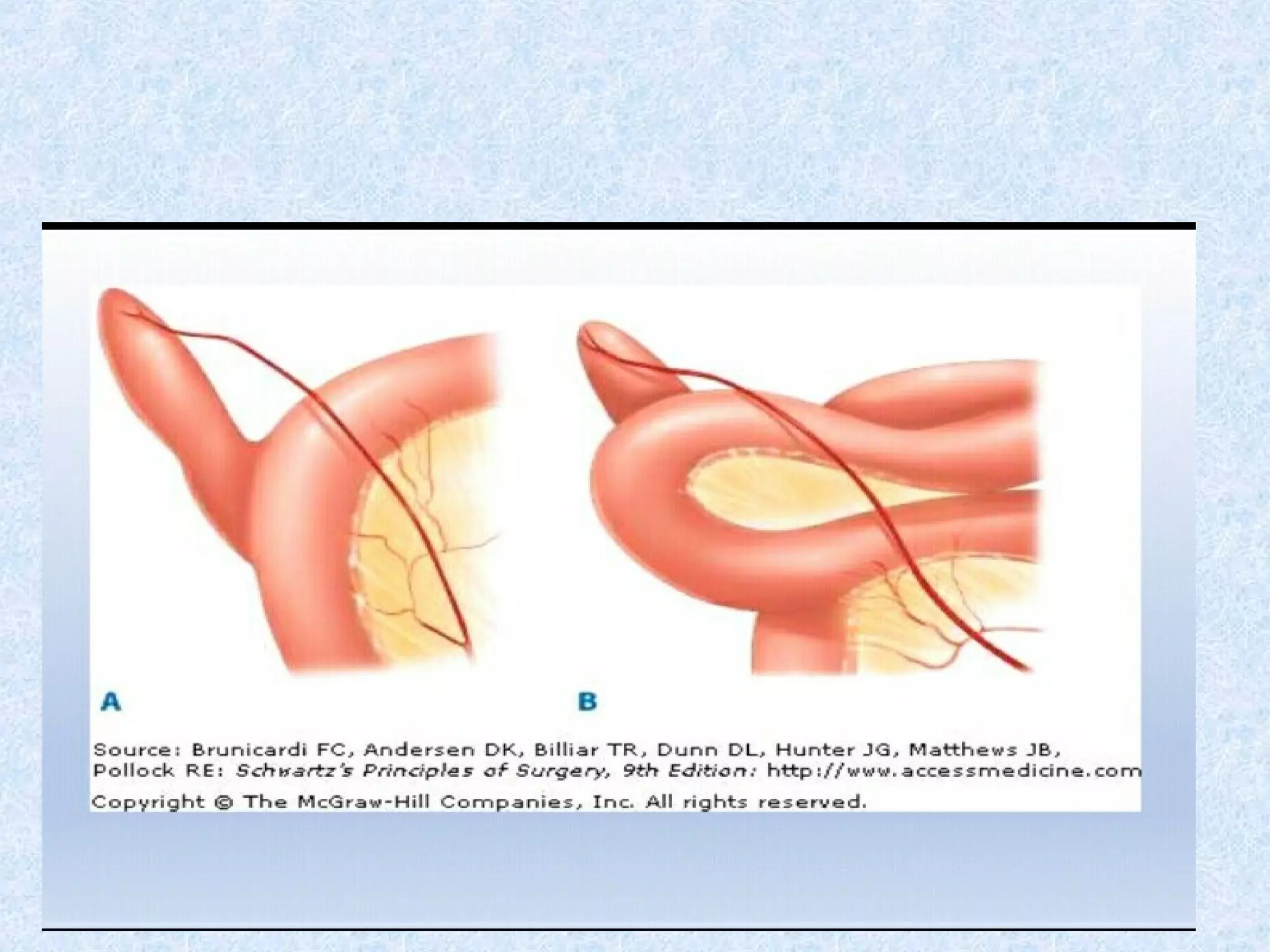
Introduction: Intestinal obstruction in toddlers presents a diagnostic dilemma, with common causes being intussusception, hernias and congenital anomalies. Meckel’s diverticulum, though a common congenital anomaly, typically presents with painless rectal bleeding. Its complications, like a persistent vitellointestinal band (Meckel’s band), causing acute mechanical obstruction are a rarer clinical entity.
Case Presentation: We report a case of a 16-month old female who presented with a 7-days history of progressive abdominal distension, 4 days of bilious vomiting and 4 days of absolute constipation. Digital rectal examination revealed finger stained with blood, initially raising suspicion for intussusception.
Management and outcome: Emergency laparotomy revealed a congenital band extending from a Meckel’s diverticulum to the umbilicus, causing a closed loop obstruction of the distal ileum. A wedge resection of the diverticulum with ileo-transverse anastomosis was performed. The postoperative course was uneventful. The patient was managed with nothing per oral and intravenous fluid for 5 days, with a drain in situ. She was discharged on the 6th postoperative day in good health, with no wound infection.
Conclusion: This case underscores that while intussusception is a prime consideration in a toddler with intestinal obstruction and rectal bleeding, congenital bands from a Meckel’s diverticulum must remain a vital differential diagnosis. A high index of suspicion and timely surgical intervention are crucial for a favorable outcome.


শিশুতে অন্ত্রের বাধা: মেকেলের ব্যান্ডের কারণে এক ঘটনা
👶 ঘটনার সারসংক্ষেপ: একজন ১৬ মাস বয়সী মেয়েশিশু হঠাৎ করে তীব্র পেট ফাঁপা, বমি (সবুজাভ/পিত্ত মিশ্রিত), এবং কয়েকদিন ধরে মল না হওয়ার সমস্যায় ভুগছিল। ডাক্তাররা প্রথমে ভেবেছিলেন এটি ইনটুসাসেপশন (অন্ত্রের ভেতরে অন্ত্র ঢুকে যাওয়া), কারণ শিশুর মলদ্বার পরীক্ষা করলে রক্ত মিশ্রিত শ্লেষ্মা পাওয়া যায়।
🔎 অপারেশনে কী পাওয়া গেল: শিশুর পেটে অস্ত্রোপচার করলে দেখা যায় একটি জন্মগত ফাইবার ব্যান্ড (মেকেলের ব্যান্ড) মেকেলের ডাইভার্টিকুলাম থেকে নাভির দিকে গিয়েছে। এই ব্যান্ডের নিচে অন্ত্র আটকে গিয়ে সম্পূর্ণ ব্লক হয়ে যায় এবং কিছু অংশে অন্ত্র নষ্ট হয়ে গেছে।
⚕️ চিকিৎসা: ব্যান্ড কেটে ফেলা হয়। মেকেলের ডাইভার্টিকুলাম অংশ কেটে বাদ দেওয়া হয়। নষ্ট হওয়া অন্ত্রের অংশ কেটে ফেলে সুস্থ অন্ত্রের সাথে জোড়া লাগানো হয়। অস্ত্রোপচারের পর শিশুটি দ্রুত সুস্থ হয়ে ওঠে এবং ৬ষ্ঠ দিনে হাসপাতাল থেকে ছাড়া পায়।
📌 মূল শিক্ষা: ছোট শিশুদের পেটে হঠাৎ বাধা হলে শুধু ইনটুসাসেপশন নয়, জন্মগত ব্যান্ড বা মেকেলের ডাইভার্টিকুলামও কারণ হতে পারে। সময়মতো অস্ত্রোপচার করলে জীবন বাঁচানো সম্ভব।


জনসচেতনতা বার্তা 🩺
ছোট শিশুদের হঠাৎ পেট ফাঁপা, বমি (বিশেষ করে সবুজাভ বা পিত্ত মিশ্রিত), এবং কয়েকদিন ধরে মল না হওয়া অন্ত্রে বাধার লক্ষণ হতে পারে। অনেক সময় ডাক্তাররা প্রথমে মনে করেন এটি ইনটুসাসেপশন, কিন্তু কিছু ক্ষেত্রে জন্মগত অস্বাভাবিকতা যেমন মেকেলের ব্যান্ড অন্ত্রকে আটকে দিয়ে মারাত্মক বাধা সৃষ্টি করতে পারে। এই অবস্থায় অন্ত্র দ্রুত নষ্ট হয়ে যেতে পারে।
⚠️ কি করতে হবে: শিশুর পেটে হঠাৎ ফাঁপা, বমি, মল না হওয়া বা রক্ত মিশ্রিত শ্লেষ্মা দেখা দিলে দেরি না করে দ্রুত হাসপাতালে নিয়ে যান। সময়মতো অস্ত্রোপচার করলে শিশুর জীবন বাঁচানো সম্ভব।
💡 মূল বার্তা: শিশুর পেটের সমস্যাকে হালকাভাবে নেবেন না। দ্রুত চিকিৎসা নিলে জটিলতা এড়ানো যায়।
2.2. Clinical History: The parents reported a 7 days history of increasing abdominal distension, associated with irritability and poor feeding and intermittent crying. This progressed to bilious vomiting for the last 4 days. There was no passage of stool for 4 days only few blood stained mucous like material came out. There was no history of fever, trauma, diarrhoea or similar episodes in the past.
2.3. Clinical findings: On examination: The child was irritable, tachycardiac and mildly dehydrated. The abdomen was markedly distended later, tense and tender on palpation, with no palpable mass. Bowel sounds were hyperactive initially but become sluggish later. Digital Rectal Examination: Revealed an empty rectal ampulla with the examining finger stained with mucous mixed blood.
2.4. Diagnostic Assessment: Based on the clinical triad of abdominal distension, bilious vomiting and constipation, a diagnosis of acute intestinal obstruction was made. The finding of blood on DRE, along with the age of the patient, made intussusception the leading preoperative diagnosis. An abdominal ultrasound was performed which shows no target sign but revealed dilated small bowel loops with fluid level. Given the clinical picture of complete obstruction, the decision was made for an emergency exploratory laparotomy.
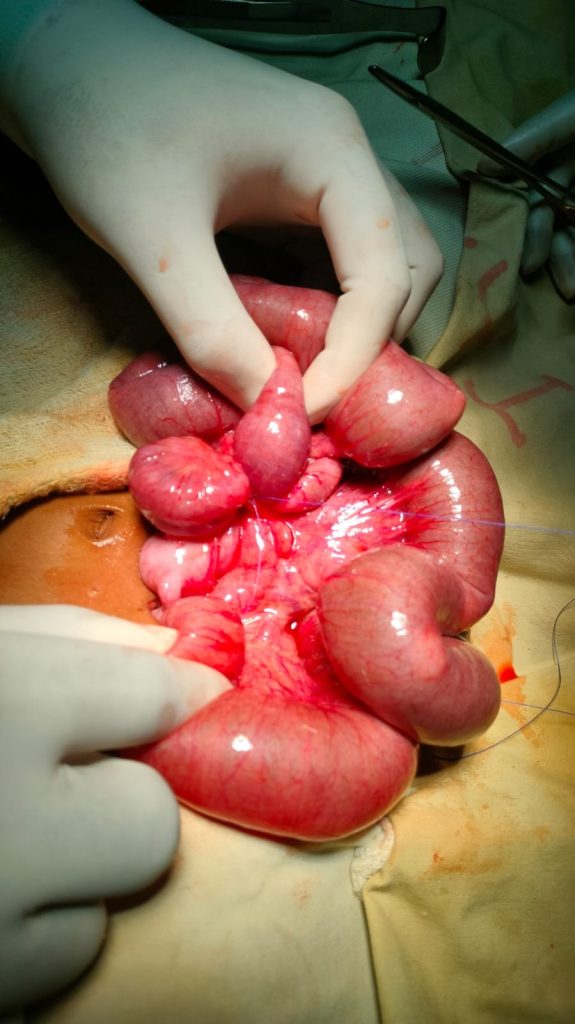
2.5. Therapeutic Intervention: A Transverse supraumbilical (Rt) incision was given. Intraoperative findings revealed a grossly dilated proximal small bowel and collapsed distal bowel. A fibrous band (Meckel’s band) was identified, extending from the tip of a Meckel’s diverticulum to the mesentery. A loop of distal ileum was entrapped under this band, causing a tight, closed loop obstruction. There was no evidence of intussusception but bowel was necrosed at the part where fibrous band compressed the gut which is about 5 cm proximal to the ileo-cecal valve. The band was lysed. A wedge resection of the Meckel’s diverticulum at its base on the antimesenteric border was performed, followed by resection of the gangrenous part upto ascending colon and end to end anastomosis was done. A drain was placed in the pelvis.
The pathophysiology involves the persistence of the omphalomesenteric duct as a fibrous cord, creating a fixed point around which small bowel loops can twist or become directly entrapped, as seen in this case. This can lead to rapid progression to strangulation and necrosis, making early intervention critical. The management is always surgical. The standard procedure involves laparotomy, lysis of band and resection of diverticulum. The choice of anastomosis depends upon the local condition of bowel and surgeon preference. An ileo-transverse anastomosis ,as performed here, is a safe option to avoid tension and narrowing at the resection site.
The key learning points are:
· Differential diagnosis: In any child with intestinal obstruction, congenital bands, including those from Meckel’s diverticulum, should be considered even when presentation suggests a more common condition like intussusception.
· Importance of exploration: When clinical and simple radiographic evidence points to complete obstruction, timely laparotomy remains both diagnostic and therapeutic.
· Surgical strategy: Simple band division with diverticulectomy and careful anastomosis provides an excellent outcome, as demonstrated by the patient’s uneventful recovery.